
PROSTATE
WIN REMARKABLE OPPORTUNITIES
BY FOLLOWING SPONSORS LINKS
EPIDEMIOLOGY
Approximately 1 in 11 men develop
prostate cancer, and 80% of cases are in men over age 65.
An estimated 221,000 new cases will be diagnosed each year, with 29,000 annual deaths as a result. African American men have the highest incidence of the disease in the United States.(reference)
An estimated 221,000 new cases will be diagnosed each year, with 29,000 annual deaths as a result. African American men have the highest incidence of the disease in the United States.(reference)
ETIOLOGY
Causative factors are unknown, but
the primary risk factor is age.
The secondary risk factor is race, with African males being more susceptible to the disease.(reference)
The secondary risk factor is race, with African males being more susceptible to the disease.(reference)
loading Favorite Sites...
SIGN & SYMPTOMS
Localized prostate cancer is
usually asymptomatic and is diagnosed through PSA test or,
less commonly, through rectal exam.
Larger tumors may produce urethral obstruction, resulting in frequent, hesitant, narrow stream urination, or nocturia. T1 or T2 tumors may be diagnosed at transurethral resection of the prostate, also known as TURP.
less commonly, through rectal exam.
Larger tumors may produce urethral obstruction, resulting in frequent, hesitant, narrow stream urination, or nocturia. T1 or T2 tumors may be diagnosed at transurethral resection of the prostate, also known as TURP.
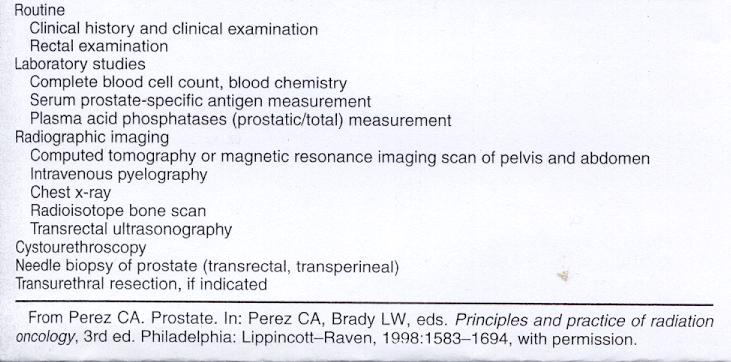
DIAGNOSE PROCEDURE
HISTOLOGY
Adenocarcinoma is the most common tumor in the prostate.
- Periurethral Duct Carcinoma (ca)
- Ductal adenocarcinoma rarely arises from the major ducts
- Transitional cell ca of the prostate is rare
- Neuroendocrine tumors are a rare variant of a malignant tumor compsed of small or carcinoid-like cells.
- Mucinous ca has been reported
- Sarcomatoid, a rare tumor that is difficult to distinguish from a true sarcoma
- Adenoid cystic ca is extremely rare in the prostate ( less than 0.1% of all tumors of this gland)
- Squamos cell ca is extremely rare
- Sarcomas (leiomyosarcoma, rhabdomyosarcoma, or fibrosarcoma) constitute approximately 0.1% of all primary neoplasms of the prostate
- Primary lymphoma of the prostate is extremely rare(reference)
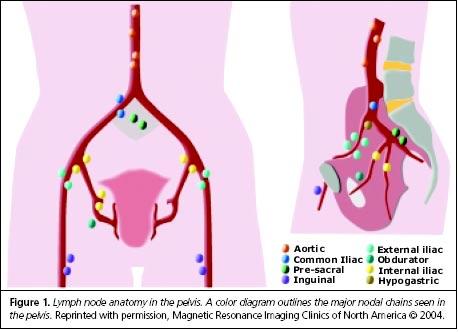
LYMPH NODE DRAINAGE
Pevlis lymph nodes to be irradiated in the pelvis with the exception of the para-aortics.(reference)
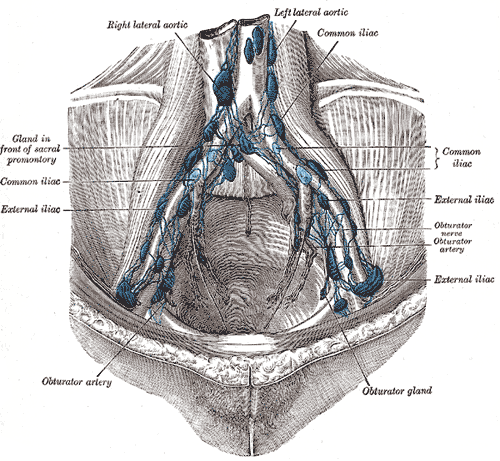
Figure 2
METASTATIC SPREAD
Prostate usually spreads to bone, lung, liver, and brain (reference)
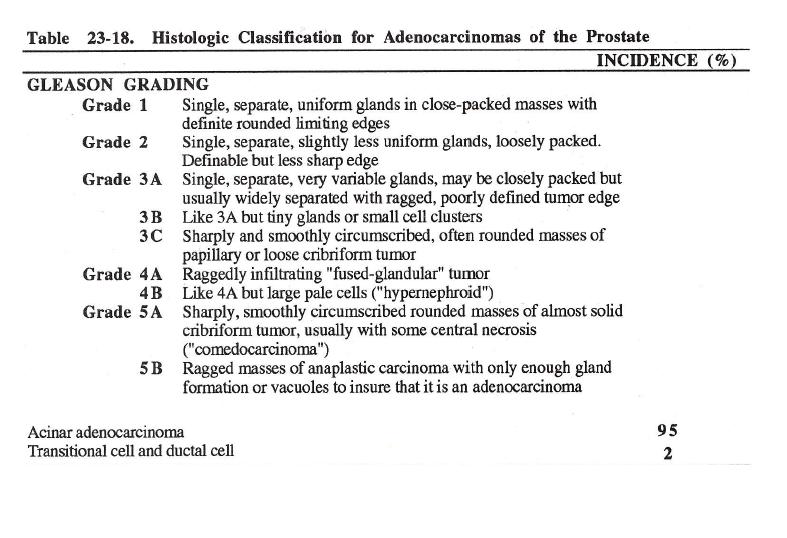
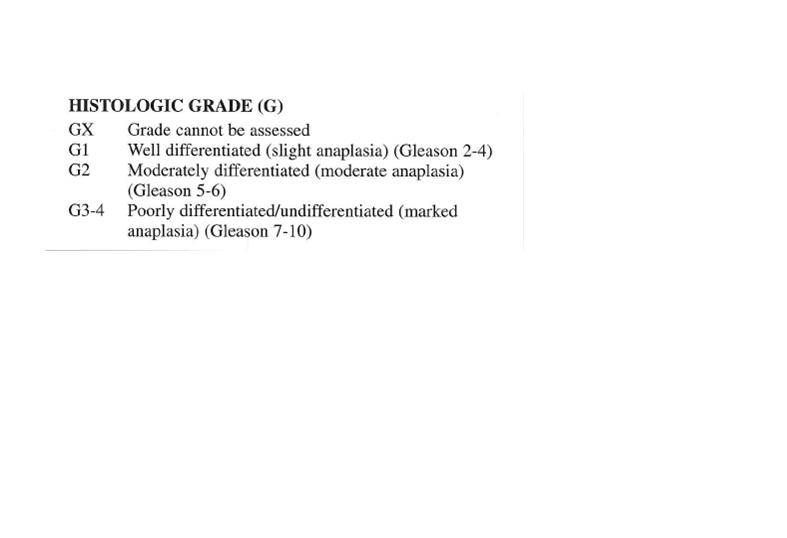
GRADING
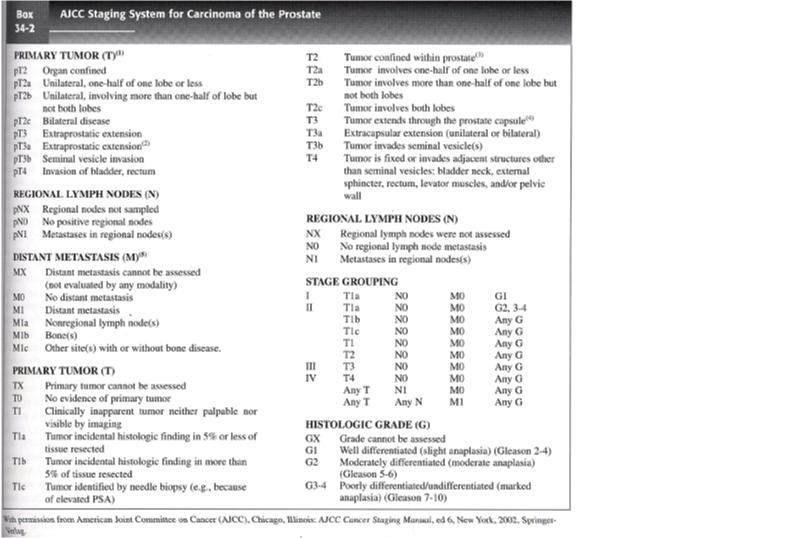
STAGING
RADIATION SIDE EFFECTS
According to Chao, et.al.,
Acute effects encompass
loose stool, diarrhea, rectal discomfort rectal bleeding, dysuria, frequency of urination, nocturia,
urinary tract infections. There is possible erythema and skin desquamation could occur in the intergluteal fold or perineum.
Less frequently:
incontinence, anal sphincter weakening and urethral stricture. Erectile dysfunction can occur in up to 50% of patients. Lumbar plexopathy is rare.
Acute effects encompass
loose stool, diarrhea, rectal discomfort rectal bleeding, dysuria, frequency of urination, nocturia,
urinary tract infections. There is possible erythema and skin desquamation could occur in the intergluteal fold or perineum.
Less frequently:
incontinence, anal sphincter weakening and urethral stricture. Erectile dysfunction can occur in up to 50% of patients. Lumbar plexopathy is rare.
PROGNOSIS
The most important indicators of
prognosis are tumor differention, stage and PSA level before treatment.
Gleason score greater than 7 indicates a poor prognosis. Persistent
disease after treatment is indicated by rising PSA levels. DNA
aneuploidy indicates aggressive disease. Region and multi-foci in the
lymph nodes denotes worse prognosis.
loading Favorite Sites...
TREATMENT
Treatment of prostate cancer can
involve, surgery, hormone therapy and irradiation. Irradiation and
surgery have comparable success rates.
All three of these treatment modalities can be used independently or in
conjunction with with each other.
Homone therapy plays a large role in the treatment of metastatic disease.4
Surgical treatment involves a radical prostatctomy, with or without post-operative radiation therapy.
The goal of hormone therpay is to either ablate the tissue which produces androgen or block the pathways for the stimulation and use of androgen.5 Before the use of any hormone therapy male breast tissue must be irradiated in order to prevent gynecomastia and the dose is usually 10 Gy in a single fraction.6
Irradiation of the prostate can come in two forms, external beam or interstitial.
Most external beam treatment today uses 3D or IMRT in order to spare normal tissue and give a conformal dose to the treatment site. Rotational fields and 4 field box plans have also been used to treat prostate cancer.7 Although not common anymore,
Tthe 4 field box would have borders
Inferior :at the bottom of the ishcial tuberosities, 1-2 cm lateral to the bony pelvis and 1.5 cm posterior to the projection of the pubic symphysis.
Although 3D fields can be of any angle, coplanar or noncoplanar, a typical arrangement for treatment of the prostate would be two anteroposterior oblique fields, two posteroanterior oblique fields and two lateral fields, all coplanar. The typical margin of the field around the PTV would be 0.8 cm.10
IMRT fields can vary greatly in the number used according to the treatment facility.
External beam radiation doses are normally 70-74 Gy given in 180-200 cGy fractions and if pelvic or periaortic lymph nodes are irradiated, 45 Gy is used with a boost to the prostate of 22-26 Gy and a boost to the nodes of 5 Gy. Post-operative radiation may be administered to the prostate using 4 field, 3D or IMRT fields when the surgical margins are positive with a typical dose of 66 Gy using a 0.8 cm field margin around the PTV.
Recommendations for the use of interstitial implants as primary therapy are as follows:
stage T1 or T2, Gleason score less than 6 and pre-treatment PSA less than 10 ng/ml.
For patients with T1 or T2, Gleason score greater than 7 or a PSA higher than 10 ng/ml, interstitial implants are combined with external beam therapy, having a dose of 40-45 Gy.14 The permanent seed implants currently use I-125 or pallaium 103 and high dose rate brachytherapy uses Ir-192.
The typical doses for permanent implants are 145 Gy for I-125, 125-135 Gy for palladium 103 and 38 Gy in
4 fractions for the HDR Ir-192.16 When the implants are combined with external beam pelvic irradiation the doses are 110 Gy for I-125, 100 Gy for palladium 103 and 20 Gy in 2 fractions for HDR Ir-192.
Homone therapy plays a large role in the treatment of metastatic disease.4
Surgical treatment involves a radical prostatctomy, with or without post-operative radiation therapy.
The goal of hormone therpay is to either ablate the tissue which produces androgen or block the pathways for the stimulation and use of androgen.5 Before the use of any hormone therapy male breast tissue must be irradiated in order to prevent gynecomastia and the dose is usually 10 Gy in a single fraction.6
Irradiation of the prostate can come in two forms, external beam or interstitial.
Most external beam treatment today uses 3D or IMRT in order to spare normal tissue and give a conformal dose to the treatment site. Rotational fields and 4 field box plans have also been used to treat prostate cancer.7 Although not common anymore,
Tthe 4 field box would have borders
Inferior :at the bottom of the ishcial tuberosities, 1-2 cm lateral to the bony pelvis and 1.5 cm posterior to the projection of the pubic symphysis.
Although 3D fields can be of any angle, coplanar or noncoplanar, a typical arrangement for treatment of the prostate would be two anteroposterior oblique fields, two posteroanterior oblique fields and two lateral fields, all coplanar. The typical margin of the field around the PTV would be 0.8 cm.10
IMRT fields can vary greatly in the number used according to the treatment facility.
External beam radiation doses are normally 70-74 Gy given in 180-200 cGy fractions and if pelvic or periaortic lymph nodes are irradiated, 45 Gy is used with a boost to the prostate of 22-26 Gy and a boost to the nodes of 5 Gy. Post-operative radiation may be administered to the prostate using 4 field, 3D or IMRT fields when the surgical margins are positive with a typical dose of 66 Gy using a 0.8 cm field margin around the PTV.
Recommendations for the use of interstitial implants as primary therapy are as follows:
stage T1 or T2, Gleason score less than 6 and pre-treatment PSA less than 10 ng/ml.
For patients with T1 or T2, Gleason score greater than 7 or a PSA higher than 10 ng/ml, interstitial implants are combined with external beam therapy, having a dose of 40-45 Gy.14 The permanent seed implants currently use I-125 or pallaium 103 and high dose rate brachytherapy uses Ir-192.
The typical doses for permanent implants are 145 Gy for I-125, 125-135 Gy for palladium 103 and 38 Gy in
4 fractions for the HDR Ir-192.16 When the implants are combined with external beam pelvic irradiation the doses are 110 Gy for I-125, 100 Gy for palladium 103 and 20 Gy in 2 fractions for HDR Ir-192.
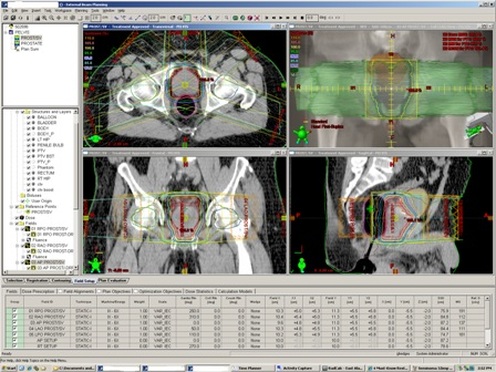
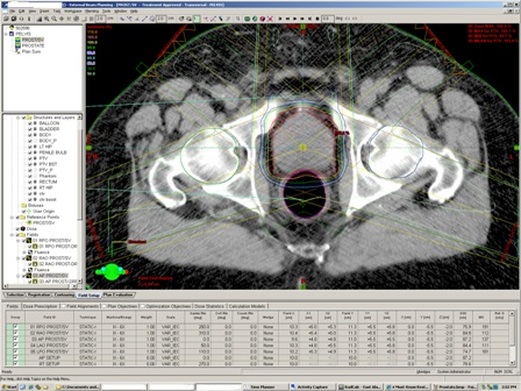
PLANING PICTURES


TD5/5
Organ Volume- 1/3(Gy) Small Intestine-50, Colon-55. Whole Organ- bladder-55,
Rectum-60, Sm.Intestine-40, Colon-40²⁴
Rectum-60, Sm.Intestine-40, Colon-40²⁴
