
ESOPHAGUS
EPIDEMIOLOGY
Most commonly a disease
of the older population, rare in>25 years old. Estimated squamous
incidence in each third of the esophagus is as follows :
Upper third 10-25%
Middle third, 40-50% L
Lower third 25-50%.
5% incidence due to "Achalasia" of >=25 years.1% (references)
Upper third 10-25%
Middle third, 40-50% L
Lower third 25-50%.
5% incidence due to "Achalasia" of >=25 years.1% (references)
ETIOLOGY
Risk factors for squamous cell :
Alcohol,
Tobacco,
Dietary factors,
more than 25 years of Achalasia, and caustic burns (especially lye corrosion).
Risk facors for adenocarcinoma :
Barrett's esophagus
Chronic esophageal reflux. (references)
Alcohol,
Tobacco,
Dietary factors,
more than 25 years of Achalasia, and caustic burns (especially lye corrosion).
Risk facors for adenocarcinoma :
Barrett's esophagus
Chronic esophageal reflux. (references)
SIGN & SYMPTOMS
Symptoms usually start 3 or 4 months
before diagnosis.
Dysphagia and Weight loss are seen in over 90% of patients.
Odynophagia (pain on swallowing) is present in up to 50% of patients.(references)
Dysphagia and Weight loss are seen in over 90% of patients.
Odynophagia (pain on swallowing) is present in up to 50% of patients.(references)
loading Favorite Sites...
DIAGNOSTIC PROCEDURES
The diagnostic workup according to
Chao is the following order.
First, a history and physical is taken of the patient.
Second, a Double contrast esophagram is done in diagnostics.
Third, a endoscopy is done along with a brushing.
Fourth, a CT or MRI are done. CT has an accuracy of 51-70% chance of detecting mediastinal nodes and about a 79% of finding left gastric or celiac node involvement. However, if CT is combined with PET scan the opportunity to diagnos metastasis sooner is of greater chance.
Fifth, a patient would get a routine chest x-ray along with labs. Then an endoscopic ultrasound would be performed to evaluate if it is limited to the esophagus or not.
Finally, this would help determine which route the patient is suggested to go for treatment. (references)
First, a history and physical is taken of the patient.
Second, a Double contrast esophagram is done in diagnostics.
Third, a endoscopy is done along with a brushing.
Fourth, a CT or MRI are done. CT has an accuracy of 51-70% chance of detecting mediastinal nodes and about a 79% of finding left gastric or celiac node involvement. However, if CT is combined with PET scan the opportunity to diagnos metastasis sooner is of greater chance.
Fifth, a patient would get a routine chest x-ray along with labs. Then an endoscopic ultrasound would be performed to evaluate if it is limited to the esophagus or not.
Finally, this would help determine which route the patient is suggested to go for treatment. (references)
HISTOLOGY
The histology of the
esophagus includes
Squamous cell carcinoma,
Adenocarcinoma, Adenoid cystic carcinoma,
Mucoepidermoid carcinoma, Adenosquamous carcinoma, and
Undifferentiated carcinoma.(references)
Squamous cell carcinoma,
Adenocarcinoma, Adenoid cystic carcinoma,
Mucoepidermoid carcinoma, Adenosquamous carcinoma, and
Undifferentiated carcinoma.(references)
LYMPH NODE DRAINAGE
"The esophagus has a dual
longitudinal interconnecting system of lymphatics."
The entire esophagus is at risk for lymphatic metastasis. The esophagus has the ability to "skip areas" up to about 8cm from origination of the tumor to where it has metastasized to. Also, up to 70% of patients were to have metastasis found at the time of autopsy. (references)
The entire esophagus is at risk for lymphatic metastasis. The esophagus has the ability to "skip areas" up to about 8cm from origination of the tumor to where it has metastasized to. Also, up to 70% of patients were to have metastasis found at the time of autopsy. (references)
METASTATIC SPREAD
According to Chao, et. al., 80% of
patient's have locally extensive and/or metastatic disease at the time
of presentation.
Local extension from cervical esophagus : larynx, trachea, prevertebral fascia
Local extension from upper thoracic esophagus : aorta, trachea, pre vertebral fascia
Local extension from mid thoracic esophagus : aorta, pericardium, left main stem bronchus,
prevertebral fascia;
Local extension from lower thoracic esophagus : aorta, pericardium diaphragm, pre vertebral fascia.
The typical sites of metastatic disease are and percentage of involvement are as follows:
45% to the abdominal lymph nodes
35% to the liver
20% to the lung
18% to the supra clavicular region
9% to bone and
5% to the adrenal glands (reference)
Local extension from cervical esophagus : larynx, trachea, prevertebral fascia
Local extension from upper thoracic esophagus : aorta, trachea, pre vertebral fascia
Local extension from mid thoracic esophagus : aorta, pericardium, left main stem bronchus,
prevertebral fascia;
Local extension from lower thoracic esophagus : aorta, pericardium diaphragm, pre vertebral fascia.
The typical sites of metastatic disease are and percentage of involvement are as follows:
45% to the abdominal lymph nodes
35% to the liver
20% to the lung
18% to the supra clavicular region
9% to bone and
5% to the adrenal glands (reference)
GRADING
General grading system recommended
by the American Joint Committee on Cancer and the International Union
Against Cancer is based on the degree of cell differentiation
Grade 1: low grade, cells well-differentiated
Grade 2: moderate grade, cells moderately differentiated.
Grade 3: high grade, cells undifferentiated
There is also a classification of that the grade can't be assessed.(reference)
Adenocarcinoma of the esopahgus possibly progresses from gasteroenteral reflux disease to Barrett's metaplasia to low-grade dysplasia to high-grade dysplasia to adenocarcinoma.( reference)
Grade 1: low grade, cells well-differentiated
Grade 2: moderate grade, cells moderately differentiated.
Grade 3: high grade, cells undifferentiated
There is also a classification of that the grade can't be assessed.(reference)
Adenocarcinoma of the esopahgus possibly progresses from gasteroenteral reflux disease to Barrett's metaplasia to low-grade dysplasia to high-grade dysplasia to adenocarcinoma.( reference)
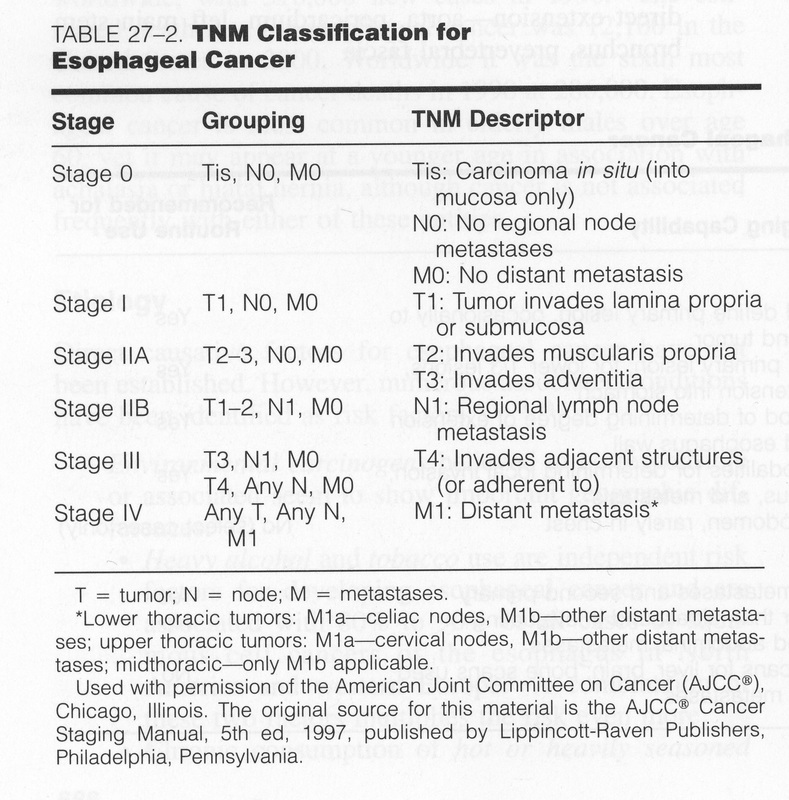
STAGING
In 1997, the American Joint Committee on Cancer, updated the TNM staging system for cancers of esophagus
RADIATION SIDE EFFECTS
Side effects of radiation therapy may include
- Skin changes -- ranging from something like a sunburn to blistering and open sores
- Nausea and vomiting
- Diarrhea
- Fatigue
- Painful sores in the mouth and throat
PROGNOSIS
Esophageal cancer usually manifest as advanced stage disease. 75%
of patients have disease lymph nodes at initial presentation. The 5
year survival rate is only 3% for these patients, whereas it is 42% for
patients who do not have nodal involvement.
Approximately 18% of patients will have distant metastases, typically to
Abdominal lymph nodes (45% of cases).
Liver (35%),
Lung (20%),
Supra clavicular nodes (18%),
Bone (9%), or Adrenal glands (5%). Consequently, the prognosis is poor, with surgical cure achieved in less than 10% of patients.Upper 1/3 lesions do better than those in the lower 1/3.
Tumors 5cm or smaller are 40% resectable, while tumors larger than 5cm have a 75% chance of distant metastasis.(reference)
In general, the prognosis of esophageal cancer is quite poor, because so many patients present with advanced disease. The overall five-year survival rate (5YSR) is less than 5%.
Individualized prognosis depends largely on stage. Those with cancer restricted entirely to the esophageal mucosa have about an 80% 5YSR, but submucosal involvement brings this down to less than 50%. Extension into the muscularis propria (muscular layer of the esophagus) has meant a 20% 5YSR and extension to the structures adjacent to the esophagus results in a 7% 5YSR.
Patients with distant metastases (who are not candidates for curative surgery) have a less than 3% 5YSR. Of all patients undergoing surgery with curative intent, the 5YSR is only about 25%(reference)
Approximately 18% of patients will have distant metastases, typically to
Abdominal lymph nodes (45% of cases).
Liver (35%),
Lung (20%),
Supra clavicular nodes (18%),
Bone (9%), or Adrenal glands (5%). Consequently, the prognosis is poor, with surgical cure achieved in less than 10% of patients.Upper 1/3 lesions do better than those in the lower 1/3.
Tumors 5cm or smaller are 40% resectable, while tumors larger than 5cm have a 75% chance of distant metastasis.(reference)
In general, the prognosis of esophageal cancer is quite poor, because so many patients present with advanced disease. The overall five-year survival rate (5YSR) is less than 5%.
Individualized prognosis depends largely on stage. Those with cancer restricted entirely to the esophageal mucosa have about an 80% 5YSR, but submucosal involvement brings this down to less than 50%. Extension into the muscularis propria (muscular layer of the esophagus) has meant a 20% 5YSR and extension to the structures adjacent to the esophagus results in a 7% 5YSR.
Patients with distant metastases (who are not candidates for curative surgery) have a less than 3% 5YSR. Of all patients undergoing surgery with curative intent, the 5YSR is only about 25%(reference)
loading Favorite Sites...
TREATMENT
The
options for treatment of cancer of the esophagus include surgery,
chemotherapy, and radiation therapy. Other treatments, such as
endoscopic mucosal resection, radiofrequency ablation, and photodynamic
therapy, may be used for early cancers and precancers of the esophagus.
Some of these treatments can also be used as palliative treatment when
all the cancer cannot be removed. Palliative treatment is meant to
relieve symptoms, such as pain and trouble swallowing, but is not
expected to cure the cancer. Depending on the stage of the cancer and
your general medical condition, different treatment options may be used
alone or in combination
Radiation Treatment with field margin of 0.5 to 0.6 cm, above and below the tumor, generally is recommended.some recommend placing the patient in the prone position for treatment to move the esophagus away from the spinal cord.
Lesions in the upper cervical or post cricoid esophagus usually are treated from the laryngopharynx to the carina. Supra clavicular and superior mediastinal nodes are irradiated electively. this can be done with lateral parallel opposed or oblique portals to the primary tumor and a single AP field for the supra clavicular and superior mediastinal nodes.
Irradiation fields for lesions in the lower two-thirds 2/3 of the esohagus (thoracis esophagus) include the entire thoracis esophagus and bilateral supraclavicular nodes in the initail treametn volume.
The inferior margin of the initial fields always includes the esophagogastric junction and, for lower-third lesions, the celiac plexus. At lest 5cm of normal tissue id included above and below the gross disease
Doses- based on data from squamous cell carcinoma of the
Upper aerodigestive tract, 50 Gy at 1.8 to 2.0 Gy per fraction over 5 weeks should control more than 90% of sub clinical disease.
1. At least 60-70 Gy is needed for gross disease in fractions of 1.8-2.0 Gy per day, 5 days per week.
2. In addition to external beam therapy, Intra-cavitary therapy can be used as part of a radical or palliative treatment plan. The most common technique is iridium 192 after loading. In general 10-20 Gy is delivered using this technique.
3. Another method used to cone down on middle -third lesions is a 360 degree rotation.(reference)
Radiation Treatment with field margin of 0.5 to 0.6 cm, above and below the tumor, generally is recommended.some recommend placing the patient in the prone position for treatment to move the esophagus away from the spinal cord.
Lesions in the upper cervical or post cricoid esophagus usually are treated from the laryngopharynx to the carina. Supra clavicular and superior mediastinal nodes are irradiated electively. this can be done with lateral parallel opposed or oblique portals to the primary tumor and a single AP field for the supra clavicular and superior mediastinal nodes.
Irradiation fields for lesions in the lower two-thirds 2/3 of the esohagus (thoracis esophagus) include the entire thoracis esophagus and bilateral supraclavicular nodes in the initail treametn volume.
The inferior margin of the initial fields always includes the esophagogastric junction and, for lower-third lesions, the celiac plexus. At lest 5cm of normal tissue id included above and below the gross disease
Doses- based on data from squamous cell carcinoma of the
Upper aerodigestive tract, 50 Gy at 1.8 to 2.0 Gy per fraction over 5 weeks should control more than 90% of sub clinical disease.
1. At least 60-70 Gy is needed for gross disease in fractions of 1.8-2.0 Gy per day, 5 days per week.
2. In addition to external beam therapy, Intra-cavitary therapy can be used as part of a radical or palliative treatment plan. The most common technique is iridium 192 after loading. In general 10-20 Gy is delivered using this technique.
3. Another method used to cone down on middle -third lesions is a 360 degree rotation.(reference)
PLANING PICTURES
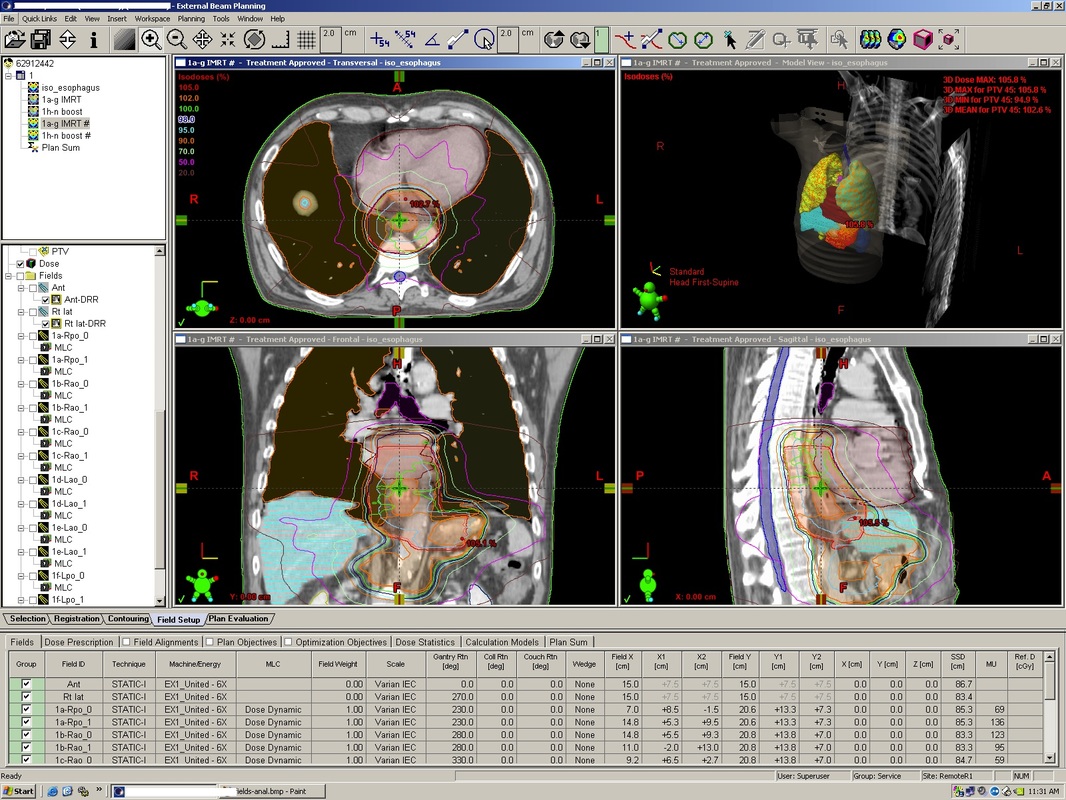
United Hospital. Eclipse planning system. Accessed January 21, 2010.
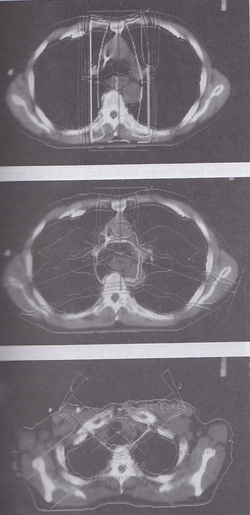
Anterior-posterior, 3 field, and wedged pair arrangements
TD5/5
Organ (1/3) (2/3), (3/3)
Esophagus 60 Gy, 58 Gy, 55 Gy
Heart 60 Gy, 45 Gy, 40 Gy
Lung 45 Gy, 30 Gy, 17.5 Gy
Spinal cord 50 Gy, 50 Gy, 47 Gy
Esophagus 60 Gy, 58 Gy, 55 Gy
Heart 60 Gy, 45 Gy, 40 Gy
Lung 45 Gy, 30 Gy, 17.5 Gy
Spinal cord 50 Gy, 50 Gy, 47 Gy
