ORAL CAVITY
WIN REMARKABLE OPPORTUNITIES
BY FOLLOWING SPONSORS LINKS
EPIDEMIOLOGY
According
to the Oral Cancer Foundation, "more than 34,000 Americans will be
diagnosed with oral cancer this year". The incidence rate is generally 2
to 4 times higher for men than women. This cancer occurs twice as often
in African Americans than in Caucasians.5
ETIOLOGY
Tobacco usage, alcohol consumption and viral infections from human papilloma virus (HPV) are contributors to the cause of oral cavity cancer. The combination of heavy smoking and drinking cause a synergistic effect that increases the risk of developing oral cancer by 15 times. Historically, 75% of oral cancer patients were smokers. Recent years have implicated HPV as a causative factor in oral cancers and increased the incidence in nonsmokers. Age is also considered a risk factor because this cancer usually occurs after the age of 40.5
SIGN & SYMPTOMS
A
sign to look for is patches inside the mouth or on the lips that are
white, a mixture of white and red, or red. White patches, leukoplakia,
are most common and sometime become malignant. Mixed red and white
patches called erythroleukoplakia are more likely than white patches to
become malignant. Red patches, erythropekia, are brightly colored,
smooth areas that often become malignant. Other signs and symptoms
include the following: a sore in the mouth or on the lip that will not
heal; bleeding in the mouth; loose teeth; difficulty or pain when
swallowing; difficulty wearing dentures; a lump in the neck; and/or an
earache.8
loading Favourite Sites...
DIAGNOSTC PROCEDURES
If
one were to detect any of the aboved mentioned signs or symptoms that
should make an appointment with their dentist or family doctor. The
doctor will do an oral exam looking at the roof and floor of the mouth,
back of the throat, and insides of the cheeks and lips. The examining
physician will look for white or red patches, lumps, swelling, or any
other abnormalities. Examination of the tongue should be done as well.
The doctor will pull the tongue outward checking its sides and
underneath. Palpation of the neck is done to ensure there are not any
swollen nodes in this area. Abnormalities are excised and a biopsy is
sent to the lab. There the pathologist reads the tissue sample. A
routine work-up is done including a history and physical and head and
neck examination.8
HISTOLOGY
Squamous Cell Carcinomas account for 90% to 95% of the histopathological types, either well or moderately differentiated.
Unusual variant types of Squamous cell carcinomas seen are verrucous carcinoma and spindle cell sqaumous cell carcinoma.4
Unusual variant types of Squamous cell carcinomas seen are verrucous carcinoma and spindle cell sqaumous cell carcinoma.4
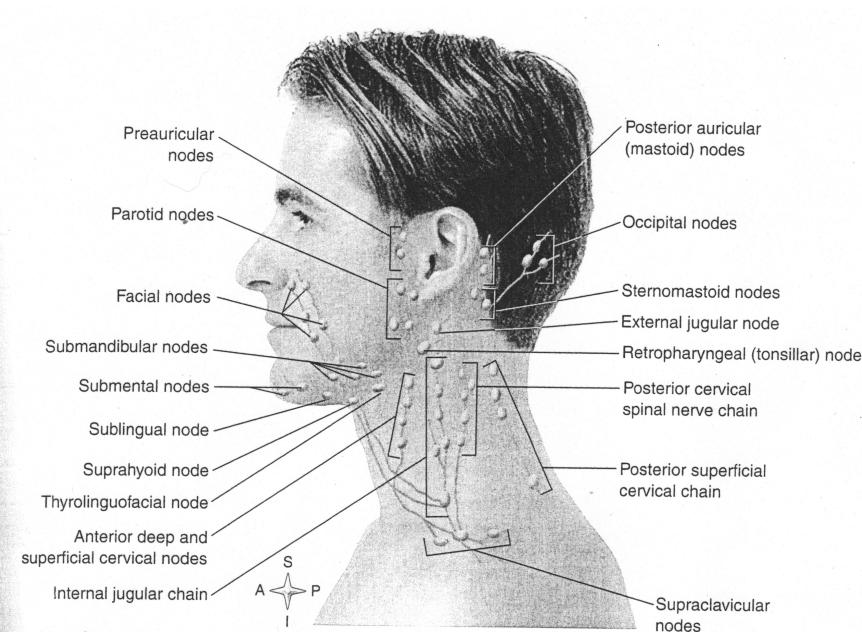
LYMPH NODE DRAINAGE
Lips: submandibular, preauricular, and facial nodes.
Buccal Mucosa: submaxillary and submental nodes
Gingiva: submaxillary and jugulodigastric nodes
Retromolar Trigone: submaxillary and Jugulodigastric nodes.
Hard palate: submaxillary and upper jugular nodes.
Floor of Mouth: submaxillary and jugular (middle and upper nodes).
Anterior two thirds of tongue: submaxillary and upper jugular nodes.4
Buccal Mucosa: submaxillary and submental nodes
Gingiva: submaxillary and jugulodigastric nodes
Retromolar Trigone: submaxillary and Jugulodigastric nodes.
Hard palate: submaxillary and upper jugular nodes.
Floor of Mouth: submaxillary and jugular (middle and upper nodes).
Anterior two thirds of tongue: submaxillary and upper jugular nodes.4
METASTATIC SPREAD
Metastatic Behavior
"Cervical lymph node involvement at the time of presentation is uncommon, and oral cavity cancer demonstrates the lowest incidence (except glottic cancer) of nodal metastasis in the head and neck region. Bloodborne spread occures in fewer than 20% of patients. Of those patients, most have cervical node involvement at the time of presentation and advanced stage disease." 4
Lung is the most common site of hematogenous spread. 2
"Cervical lymph node involvement at the time of presentation is uncommon, and oral cavity cancer demonstrates the lowest incidence (except glottic cancer) of nodal metastasis in the head and neck region. Bloodborne spread occures in fewer than 20% of patients. Of those patients, most have cervical node involvement at the time of presentation and advanced stage disease." 4
Lung is the most common site of hematogenous spread. 2
GRADING
Histopathologic grade (G)
GX - Grade not assessable
G1- Well Differentiated
G2 - Moderately differentiated
G3 - Poorly differentiated
G4 - Undifferentiated 4
GX - Grade not assessable
G1- Well Differentiated
G2 - Moderately differentiated
G3 - Poorly differentiated
G4 - Undifferentiated 4
STAGING
TNM staging by American Joint Committee on Cancer Staging
T is for Primary Tumor
TX--Primary Tumor unable to be assessed
T0--There is no evidence of the primary tumor
Tis--Carcinoma in situ
T1--The tumor is less than or equal to 2 cm in greatest dimension
T2--The tumor is greater than 2 cm but less than 4 cm in greatest dimension
T3--The tumor is greater than 4 cm in greatest dimension
T4(lip)--Tumor invades adjacent structures such as cortical bone, inferior alveolar nerve, floor of mouth, skin of face, etc.
T4(oral cavity)--Tumor invades adjacent structures such as cortical bone, deep muscle of tongue, maxillary sinus, skin
Regional Nodes
NX--Regional nodes unable to be assessed
N0--No regional metastasis
N1--Mets in a single ipsilateral node that is less than or equal to 3 cm in greatest dimension
N2-
N2a--Mets in a single ipsilateral node that is greater than 3 cm but less than 6 cm in greatest dimension
N2b--Mets in multiple ipsilateral nodes with none being greater than 6 cm
N2c--Mets in bilateral and contralateral lymph nodes with none being greater than 6 cm
N3--Mets in any lymph node greater than 6 cm
Metastasis
MX--The presence of distant mets could not be assessed
M0--No distant mets
M1--Distant mets 1
The Staging groups are as follow:
Stage 0 = Grouping Tis, N0, M0
Stage 1 = T1, N0, M0
Stage 2 = T2, N0, M0
Stage 3 = T3, N0, M0
T1, N1, M0
T2, N1, M0
T3, N1, M0
Stage 4a = T4, N0, 1, M0
Any T, N2, M0
Stage 4b = Any T, N3, M0
Stage 4c = Any T, Any N, M12
T is for Primary Tumor
TX--Primary Tumor unable to be assessed
T0--There is no evidence of the primary tumor
Tis--Carcinoma in situ
T1--The tumor is less than or equal to 2 cm in greatest dimension
T2--The tumor is greater than 2 cm but less than 4 cm in greatest dimension
T3--The tumor is greater than 4 cm in greatest dimension
T4(lip)--Tumor invades adjacent structures such as cortical bone, inferior alveolar nerve, floor of mouth, skin of face, etc.
T4(oral cavity)--Tumor invades adjacent structures such as cortical bone, deep muscle of tongue, maxillary sinus, skin
Regional Nodes
NX--Regional nodes unable to be assessed
N0--No regional metastasis
N1--Mets in a single ipsilateral node that is less than or equal to 3 cm in greatest dimension
N2-
N2a--Mets in a single ipsilateral node that is greater than 3 cm but less than 6 cm in greatest dimension
N2b--Mets in multiple ipsilateral nodes with none being greater than 6 cm
N2c--Mets in bilateral and contralateral lymph nodes with none being greater than 6 cm
N3--Mets in any lymph node greater than 6 cm
Metastasis
MX--The presence of distant mets could not be assessed
M0--No distant mets
M1--Distant mets 1
The Staging groups are as follow:
Stage 0 = Grouping Tis, N0, M0
Stage 1 = T1, N0, M0
Stage 2 = T2, N0, M0
Stage 3 = T3, N0, M0
T1, N1, M0
T2, N1, M0
T3, N1, M0
Stage 4a = T4, N0, 1, M0
Any T, N2, M0
Stage 4b = Any T, N3, M0
Stage 4c = Any T, Any N, M12
RADIATION SIDE EFFECTS
Xerostomia
(dry mouth) is common in patients receiving doses greater than 35-45Gy
to major salivary glands and the effect could last for years. Hand in
hand with xerostomia comes loss of taste. These two in combination often
lead to weight loss in patients.
Osteoradionecrosis is a major side effect (complication) seen with this type of cancer. Many problems arise from teeth that have to be extracted after radiation treatment is completed and often require the use of hyperbaric oxygen treatments. If dental extractions are carried out before treatment, it is better for the patient.²
Osteoradionecrosis is a major side effect (complication) seen with this type of cancer. Many problems arise from teeth that have to be extracted after radiation treatment is completed and often require the use of hyperbaric oxygen treatments. If dental extractions are carried out before treatment, it is better for the patient.²
PROGNOSIS
As
with all cancers, the outcome is dependent on the stage of the tumor,
and if there is nodal involvement. The 5 year survival for oral cavity
cancer (excluding lip and tongue cancers) is 47%.6
Oral cavity cancers can be difficult to control. Prognosis is poor if
the primary tumor extends into the soft tissue of skin of the neck.7
Cervical nodes status plays a big role in the survival determinant for all sites. Early primary lesions fare well, while advanced disease has a poor outlook.
Below is a chart that displays the overall 5-yr survival rates for each site and the 5-yr survival rates for each stage.²
Cervical nodes status plays a big role in the survival determinant for all sites. Early primary lesions fare well, while advanced disease has a poor outlook.
Below is a chart that displays the overall 5-yr survival rates for each site and the 5-yr survival rates for each stage.²
loading Favorite Sites...
TREATMENT
There are 3 treatment options for oral cavity cancer: surgery, radiation therapy, and/or laser excision.
Surgical Excision
Oral Tongue:
- Wide excision with 1 cm margin
- Hemi- or total glossectomy for large lesions
Floor of the Mouth:
- Lesions fixed to the mandible or advanced lesions should be excised along with segmental resection of the mandible
- Post-op radiation therapy is recommended
Radiation Therapy Techniques
External Beam:
- Opposed lateral portals include submandibular, subdigastric, and submental nodes
- Superior border needs to be 2 cm above dorsum of the tongue
- Posterior border needs to be 2 cm behind the sternocleidomastoid muscle
- Inferior border needs to be at thyroid notch
- Cervical node mets are treated with AP field with larynx shield to 4500 Gy then the posterior chain is treated with an electron energy as a boost to
spare the spinal cord
- When considering fields and dosage it is very important to minimize exposure to the manible
- If margins are close or positive or if there is any extracapsular extension in the cervical nodes an additional 6 Gy is given with reduced fields
- Dosage:
- Micoscopic Disease > 55-60 Gy
- Small T1 and T2 Tumors > 65-70 Gy
- Large T3 and T4 Tumors > Higher dose if Radiation used alone
- Post- Op > 60 Gy
Interstitial Irradiation:
- Most common technique: Pecutaneous afterloading with angiocatheters and iridium 192
- Cover tumor with .5- 1 cm margin
- Low-dose rate of 4.5- 5 Gy an hour
- Good results achieved for small T1 and T2 tumors alone or with external beam
- Local control for patients with microscopic tumor at the surgical margins
Surgical Excision
Oral Tongue:
- Wide excision with 1 cm margin
- Hemi- or total glossectomy for large lesions
Floor of the Mouth:
- Lesions fixed to the mandible or advanced lesions should be excised along with segmental resection of the mandible
- Post-op radiation therapy is recommended
Radiation Therapy Techniques
External Beam:
- Opposed lateral portals include submandibular, subdigastric, and submental nodes
- Superior border needs to be 2 cm above dorsum of the tongue
- Posterior border needs to be 2 cm behind the sternocleidomastoid muscle
- Inferior border needs to be at thyroid notch
- Cervical node mets are treated with AP field with larynx shield to 4500 Gy then the posterior chain is treated with an electron energy as a boost to
spare the spinal cord
- When considering fields and dosage it is very important to minimize exposure to the manible
- If margins are close or positive or if there is any extracapsular extension in the cervical nodes an additional 6 Gy is given with reduced fields
- Dosage:
- Micoscopic Disease > 55-60 Gy
- Small T1 and T2 Tumors > 65-70 Gy
- Large T3 and T4 Tumors > Higher dose if Radiation used alone
- Post- Op > 60 Gy
Interstitial Irradiation:
- Most common technique: Pecutaneous afterloading with angiocatheters and iridium 192
- Cover tumor with .5- 1 cm margin
- Low-dose rate of 4.5- 5 Gy an hour
- Good results achieved for small T1 and T2 tumors alone or with external beam
- Local control for patients with microscopic tumor at the surgical margins
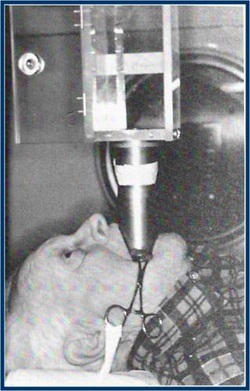
Intraoral Cone:
- Most optimal with lesions in the anterior tongue or anterior segment of the floor of the mouth
- 250 keV or electron beams of 6-12 MeV
PLANING PICTURES
Site Specific Treatment:
Lip:
-Lesions < 4cm = surgery + radiation therapy
-Lesions > 4cm = radiation therapy + surgery for salvage
-No regional nodes treated
-Target Volume = tumor + 1.5cm margins
-External beam = 100-200 keV and/or electron beam of 6-9 MeV with 1-1.5cm bolus
-Custom lead shields used to protect underlying gum and manible
-Dose = 50 Gy for small lesions, 60 Gy for larger lesions
-Interstitial irradiation is an option for smaller lesions
Oral Tongue:
-Dose = 60-65 Gy for smaller lesions sitting posteriorly, ill-defined lesions not accessible for surgical excision via the peroral route; 65-70 Gy for
superficial, exophphytic T1 and T2 lesions with little muscle involvment; 50-60 Gy for T3 and T4 lesions combined with surgery
-Intersitial implant or intraoral cone may be used to boost small lesions sitting anteriorly not involving adjacent floor of the mouth or gingival ridge an additional 25-30 Gy giving the primary lesion a total dose of 70-80 Gy
Lip:
-Lesions < 4cm = surgery + radiation therapy
-Lesions > 4cm = radiation therapy + surgery for salvage
-No regional nodes treated
-Target Volume = tumor + 1.5cm margins
-External beam = 100-200 keV and/or electron beam of 6-9 MeV with 1-1.5cm bolus
-Custom lead shields used to protect underlying gum and manible
-Dose = 50 Gy for small lesions, 60 Gy for larger lesions
-Interstitial irradiation is an option for smaller lesions
Oral Tongue:
-Dose = 60-65 Gy for smaller lesions sitting posteriorly, ill-defined lesions not accessible for surgical excision via the peroral route; 65-70 Gy for
superficial, exophphytic T1 and T2 lesions with little muscle involvment; 50-60 Gy for T3 and T4 lesions combined with surgery
-Intersitial implant or intraoral cone may be used to boost small lesions sitting anteriorly not involving adjacent floor of the mouth or gingival ridge an additional 25-30 Gy giving the primary lesion a total dose of 70-80 Gy
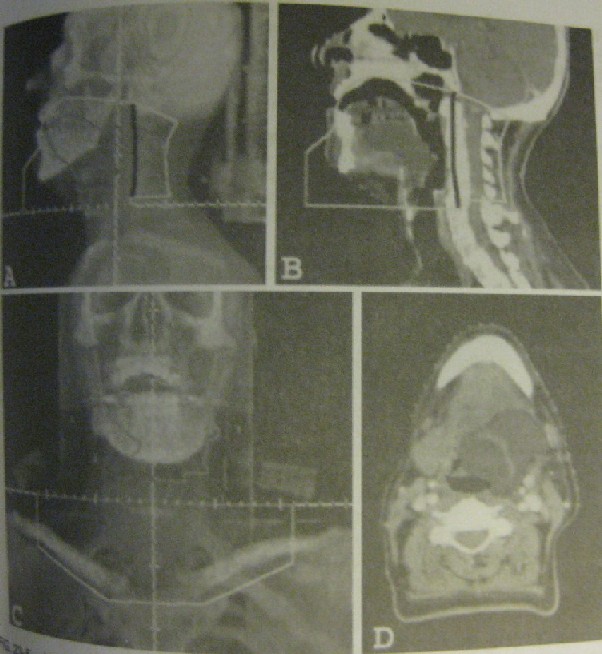
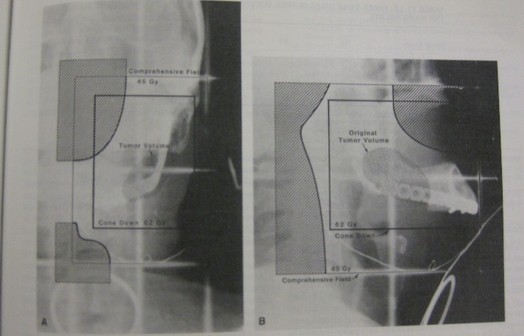
A) Digital composite radiograph showng a lt lat portal for oral tongue.
B)Sagittal view showing which structures are included in the field
C) Anterior lower neck portal
D) An axial view through the tumor to show extent of disease¹
|
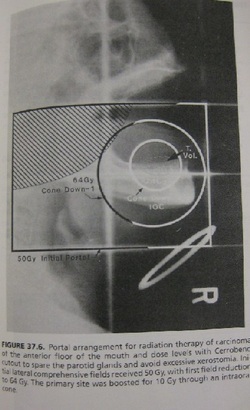
Floor of the Mouth:
-Small superficial lesions = interstitial implant (60-65 Gy) or intraoral cone (45 Gy over 3 weeks) only, no surgery required -T1 and early T2 lesions = external beam to 45 Gy then boost with interstitial implant to 70 Gy or intraoral cone to 65 Gy -Advanced T3 and T4 lesions = external beam to primary tumor and nodes to 45 Gy then reduced fields 2 or 3 times for a total dose of 7440 cGy to 7680 cGy with hyperfractionated regimen of 1.2 Gy BID |
|
Buccal Mucosa:
-Small superficial T1 lesions = surgery
-Intermediate T2 lesions and those involving the commisure = radiation therapy
-T3 and T4 lesions with deep muscular invasion = radical surgery, reconstruction, and post-op radiation therapy
-T1 and T2 lesions without nodal involvement = photon or electron beam therapy combined with interstitial implant or intraoral cone therapy
-Moderately advanced lesions with or without positive nodes = radiation therapy to primarty site and regional lymph nodes
-Tumor dose of 55-60 Gy with a boost for an additional 20 Gy
-Small superficial T1 lesions = surgery
-Intermediate T2 lesions and those involving the commisure = radiation therapy
-T3 and T4 lesions with deep muscular invasion = radical surgery, reconstruction, and post-op radiation therapy
-T1 and T2 lesions without nodal involvement = photon or electron beam therapy combined with interstitial implant or intraoral cone therapy
-Moderately advanced lesions with or without positive nodes = radiation therapy to primarty site and regional lymph nodes
-Tumor dose of 55-60 Gy with a boost for an additional 20 Gy
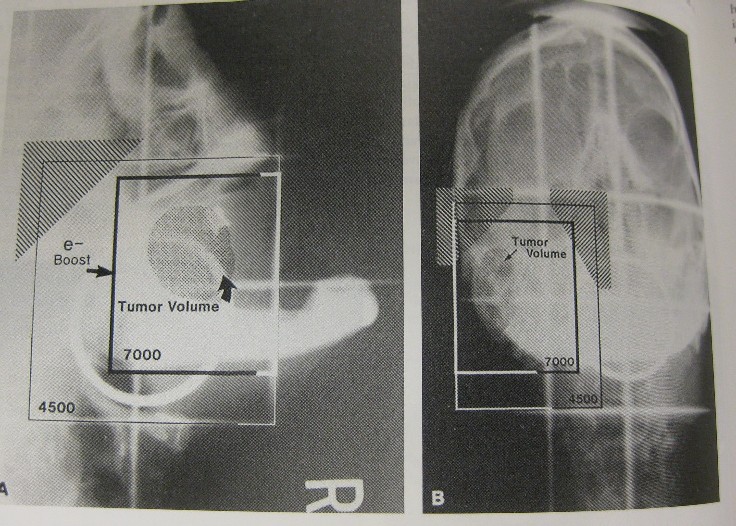
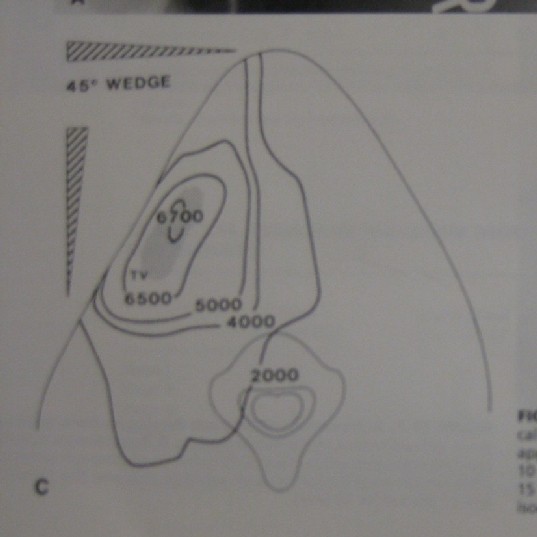
Portal arrangement for treating carcinoma of the buccal mucosa. This shows an initial anteroposterior and ipsilateral wedge pair technique to 45Gy with a field reduction for another 10Gy. Then the primary lesion was boost with 9e- for another 15Gy in 5 days.
A) Lateral view
B) AP view
C) Composite isodose lines for treatment¹°
Gingiva:
-Small T1 exophytic lesions without boney involvment = external beam only
-Portals should include entire segment of hemimandible from mental symphysis to TMJ
-Positive nodes or advanced lesions = ipsilateral treatment
-Advanced lesions with or without mets = radical surgery9
-Small T1 exophytic lesions without boney involvment = external beam only
-Portals should include entire segment of hemimandible from mental symphysis to TMJ
-Positive nodes or advanced lesions = ipsilateral treatment
-Advanced lesions with or without mets = radical surgery9
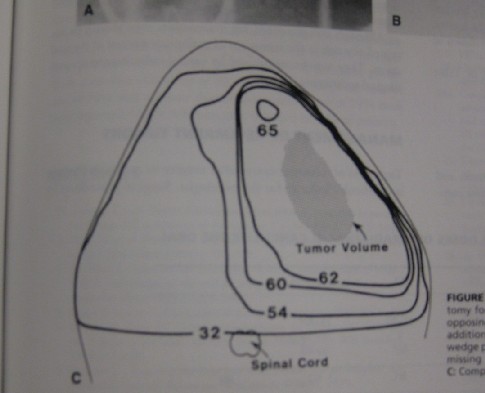
A) Anterior view of portal arrangement after hemimandibulectomy for treatment of alveolar ridge carcinoma. Consists of opposed lateral fields to 38.4Gy and a field reduction to 6.4 Gy followed by an anteroposterior and ipsilateral wedge pair approach for another 18 Gy.
B) Lateral view
C) Composite isodose lines of the treatment¹°
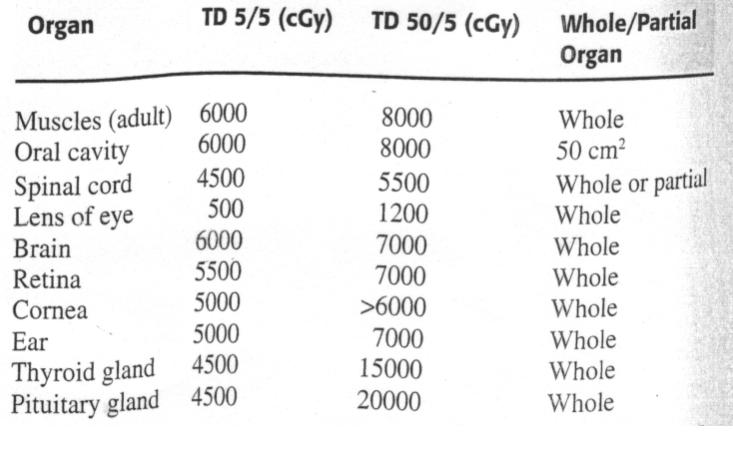
TD5/5