
BREAST
WIN REMARKABLE OPPORTUNITIES
BY FOLLOWING SPONSORS LINKS
EPIDEMIOLOGY
Inflammatory Breast Cancer (IBC) only makes up 1-6% of all breast cancer cases. IBC is usually diagnosed in younger women (average 57 years old). African-Americans are usually diagnosed at younger ages than Caucasian women and also have a higher risk of getting IBC. (Reference)
ETIOLOGY
• Advanced age and Gender
• Family history - 2 or more relatives with BC, 1st degree relative, Family history of ovarian cancer
• Personal history - Positive BRCA1/BRCA2 mutation, Breast biopsy with atypical hyperplasia, LCIS, DCI
• Reproductive history - Early age at menarche, Late age of menopause, late age of 1st term pregnancy, use
of combined estrogen/progesterone HRT, Use of oral contraceptives
• Lifestyle factors - Adult weight gain, Sedentary lifestyle, Alcohol consumption
• Family history - 2 or more relatives with BC, 1st degree relative, Family history of ovarian cancer
• Personal history - Positive BRCA1/BRCA2 mutation, Breast biopsy with atypical hyperplasia, LCIS, DCI
• Reproductive history - Early age at menarche, Late age of menopause, late age of 1st term pregnancy, use
of combined estrogen/progesterone HRT, Use of oral contraceptives
• Lifestyle factors - Adult weight gain, Sedentary lifestyle, Alcohol consumption
SIGN & SYMPTOMS
Inflammatory carcinoma can presents with rapid onset of erythema, warmth and edema.
Symptoms to look for can include:
• Pain in the breast
• Skin changes in breast
• Reddened area with texture and thickness of an orange (peau d'orange)
• Bruise that does not go away
• Sudden swelling of the breast
• Itching of the breast
• Nipple retraction (flattened look) or discharge
• Swelling of lymph nodes under the arm or in the neck
• Unusual warmth of the affected breast, Edema
• Breast is harder or firmer
• A lump may become present and grow rapidly
Symptoms to look for can include:
• Pain in the breast
• Skin changes in breast
• Reddened area with texture and thickness of an orange (peau d'orange)
• Bruise that does not go away
• Sudden swelling of the breast
• Itching of the breast
• Nipple retraction (flattened look) or discharge
• Swelling of lymph nodes under the arm or in the neck
• Unusual warmth of the affected breast, Edema
• Breast is harder or firmer
• A lump may become present and grow rapidly
loading Favorite Sites...
DIAGNOSTC PROCEDURES
Standard diagnostic tests for breast cancer such as mammograms, MR and needle biopsy generally cannot accurately diagnose IBC. The following tests are used to make a diagnnosis:⁹
•surgical biopsy - larger samples of breast skin and underlying tissue can be collected in a surgical or skin biopsy
•PET scan
•surgical biopsy - larger samples of breast skin and underlying tissue can be collected in a surgical or skin biopsy
•PET scan
HISTOLOGY
Pathologic evidence of malignancy and clinical findings of breast tenderness and enlargement, peuau d' orange appearance, erythema, warmth, and diffuse induration of the skin. "Infiltrating ductal carcinoma is the most common histologic type of breast malignancy, accounting for 70% of all breast cancers. Infiltrating lobular carcinoma is the next most common type, comprising about 5% to 10% of breast cancers." "There are several other relatively rare types of infiltrating breast cancer, such as mucinous or colloid, tubular, and papillary carcinoma. These lesions have distinct histologic characteristics and tend to yield a more favorable prognosis."⁸
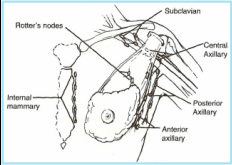
LYMPH NODE DRAINAGE
A network of lymphatics lies over the entire surface of the chest, neck and abdomen and become dense under the areola. See image below.²
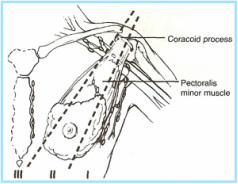
Lymphatic drainage moves superiorly
and laterally towards the axillary lymph nodes. See image below of
axillary lymph node levels.²
METASTATIC SPREAD
Lymphatic spread is most common, but breast cancer can also spread by direct invasion and by hematogenous spread.²
Lymphatic spread frequently occurs T3 and T4 lesions to the axillary, internal mammary or supraclavicular lymph nodes. Specifically for inflammatory (T4d) cases, tumor emboli are present in the dermal lymphatics. Direct extension can occur to the ribs, intercostal muscles, or skin. Hematogenous spread can occur to bone, lung, or pleura.¹,⁵
Lymphatic spread frequently occurs T3 and T4 lesions to the axillary, internal mammary or supraclavicular lymph nodes. Specifically for inflammatory (T4d) cases, tumor emboli are present in the dermal lymphatics. Direct extension can occur to the ribs, intercostal muscles, or skin. Hematogenous spread can occur to bone, lung, or pleura.¹,⁵
STAGING
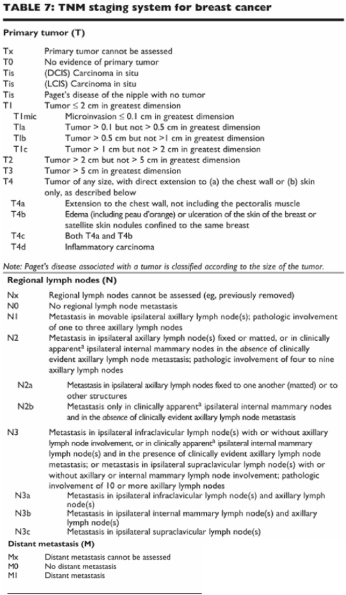
AJCC/TNM (Please see table below)³
Inflammatory breast cancer is specifically T4d¹
RADIATION SIDE EFFECTS
Radiation sequelae are related to irradiated volume, total dose, and concurrent chemotherapy. After definitive irradiation for advanced breast carcinoma at M.D. Anderson, 20% developed severe cubcutaneous fibrosis; 5% to 10% ahd rib fractures and symptomatic pneumonitis, and a lower percentage had soft tissue and skin necrosis and ulceration.¹
PROGNOSIS
Poor Prognosis. The overall 5-year survival rate regardless of disease status is 85%. The 5-year survival decreases to 77% if evidence exists of regional spread. If there is metastasis present at the time of diagnosis the 5-year survival rate decreases to 21%. Survival rates correlate with early detection, tumor characteristics, treatment approach, and the patients condition. The 10-year survival rate is 75.7% and the 15-year survival rate is 57.7%. Patients may relapse up to 20 years or more after treatment. ⁸ 5-year survival rate for patients with lesions less than .5cm is 99%, and .5cm larger is 82%. With regional lymph node metastasis, 4.5cm tumors have a 70% incidence rate of nodal involvement, whereas 1.5cm tumors have a 38% incidence rate.⁸ Location of primary tumor does not directly affect prognosis.⁸
loading Favorite Sites...
TREATMENT
General Management
Radiation Therapy Techniques
- Because of a compelling need for systemic therapy, multiagent chemotherapy plays a primary role in the treatment of these patients.
- Surgery should be performed on all patients with technically resectable disease. Borderline resectable and unresectable locally advanced breast cancers have been treated with irradiation alone.
- Neoadjuvant chemotherapy before surgical resection and irradiation plays a prominent role.
Radiation Therapy Techniques
- Patients with technically inoperable tumors should be irradiatied to the breast, supraclavicular nodes, and axillary nodes.
- Treatment of the ipsilateral internal mammary lymph nodes may be indicated if medial chestwall/breast disease is present or if there is clinical or radiaographic involvement of the internal mammary node chain.
- The breast is treated with photon through tangential fields with borders similar to those used in early breast cancer, ensuring that all potential tumor-bearing tissues are adequately covered.
- Irradiation of the chest wall after mastectomy can be accomplished with tangential photos fields (as in the intact breast) or with appositional eletron beams.
- Bolus is necessary over the entire field for part of the treatmetn, and should be added to the scar along for an additional part of the treatment.
- Several electron-beam techniques can be used as an alternative to tangential photon treatment; the simplest is a single appositional field using 6 to 12 MeV electrons. CT scans assis in determining the thickness of the chest wall to select the optimal electron beam energy. Bolus should be used for part of the treatment to increase the surface dose beyond the 80% to 90% typically given with these beams, and to minimize the lung dose.
- Anatomic landmarks defining the field borders for treatment of breast/chestwall tangentials, supraclavicular nodes, internal mammary nodes, and axilla are similar to those used to treat early breast cancer.
- Total dose to the entire breast or chest wall is 50 Gy in 1.8 to 2.0 daily fractions.
- If surgery is not feasible, the breast should be given an additional 10 to 25 Gy with external irradiaiton. This should be performed with shrinking fields to a dose of 75 to 80 Gy. The boost dose is determined by the volume of residual disease.
- In patients with close or positive margins, a boost of 10 to 15 Gy is given to a reduced volume.
- Internal mammary nodes, supraclavicular fossa nodes, and axillary nodeal areas should receive 45 to 50 Gy if no macroscopic tumor is present.
- Any gross nodal disease should be boosted with an additional 10 to 15 Gy using a reduced appositional electron beam field.
- In general, postmastectomy irradiation is recommended for lesions larger than 5 cm in diameter; any skin, fascial, or skeletal muscle involvement; poorly differentiated tumors; positive or close surgival margins; lymphatic permeation; matted lyumph nodes; two or more positive axillary lymph nodes; or gross extracapsular tumor extension.
- Adjuvant irradiation can be effectively given before, concurrent with, or after chemotherapy.¹
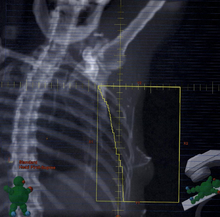
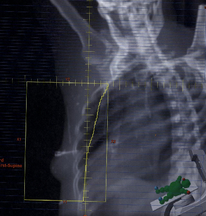
PLANING PICTURES
DRRs showing the different fields used in a mono-isocentric 5-field treatment plan for an inflammatory left breast cancer diagnosis.⁶
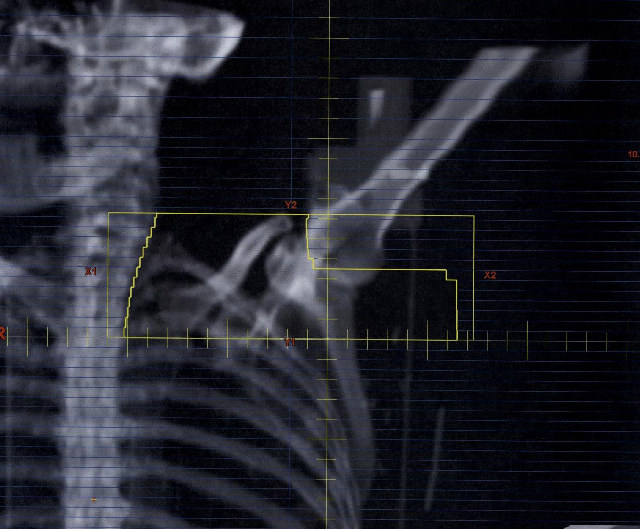
Supraclavicular Field
Medial Tangent Field
|
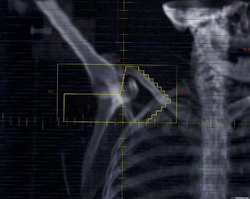
Posterior Axillary Boost Field
Lateral Tangent Field
|
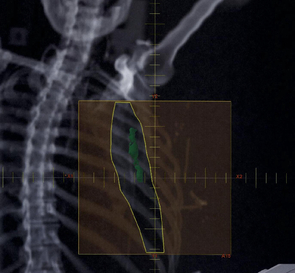
Internal Mammary Node E- field
