
NASOPHARYNX
WIN REMARKABLE OPPORTUNITIES
BY FOLLOWING SPONSORS LINKS
EPIDEMIOLOGY
H
& N tumors in general account for approximately 5% of the overall
incidence of cancer in the U.S., and 2% of all cancer deaths.Rates are
twice as high in males than in females.Higher in certain populations and
geographical regions of the world (southern China, Southeast Asia, and
Hong Kong).1
ETIOLOGY
Primary risk factors for this disease are tobacco and alcohol. Occupations associated with greater risk
factors are nickel refining, steel and textile workers. EBV and genetic host factors.1
factors are nickel refining, steel and textile workers. EBV and genetic host factors.1
SIGN & SYMPTOMS
Nasal stuffiness, dysphagia, nasal twang, decrease in hearing , ear pain., headache, and, sore throat
lump in the neck, and chronic ulcer.2
lump in the neck, and chronic ulcer.2
loading Favorite Sites...
DIAGNOSTC PROCEDURES
Typical diagnostic procedures for
nasopharyngeal cancer are the following: a complete history and
physical, nasopharyngoscopy using an endoscope and biopsy of any
suspicious tissues. Imaging studies: CT and MRI using contrast. CT is
better at delineating bone destruction from any cancer and MRI is better
at delineating soft tissue changes.3
HISTOLOGY
90% is squamous cell carcinoma (SCC) and SCC variations (epidermoid or undifferentiated carcinomas). The other 10%
are usually lymphoma.4
are usually lymphoma.4
LYMPH NODE DRAINAGE
Nodal disease can be bilateral in
up to 50% of cases. Main lymphatic drainage routes: from the
retropharyngeal nodes to the superior jugular nodes and into the
posterior cervical nodes.5
METASTATIC SPREAD
Bone (primary metastatic site), lung, liver 6
GRADING
Gx: Grade cannot be evaluated
G1: Well differentiated
G2: Moderately differentiated
G3: Poorly differentiated 7
G1: Well differentiated
G2: Moderately differentiated
G3: Poorly differentiated 7
STAGING
In 1997, the American Joint Committee on Cancer, in collaboration with the Union Internationale Contre le Cancer, updated the TNM staging system for cancers of the head and neck. Primary tumors are classified as T1 to T4.
Nodal dissease as N1,N2 or N3.
Distant metastasis is staged as M1,
and the overall stage grouping consists of stages 1 to 1V.
Stages I and II are considered to be early cancers.
Advanced stages are III and IV cancers.¹¹
Nasopharynx
T1-tumor confined to nasopharynx.
T2-tumor extends to soft tissures of oropharynx and/or nasal fossa.
T2a- Without parapharyngeal extension.
T2b-With parapharngeal extension.
T3-tumor invades bony structures and/or paranasal sinuses.
T4-Tumor with intracranial extension and/or involvement of cranial nerves, infratemporal fossa, hypopharynx, or orbit.8
Nodal dissease as N1,N2 or N3.
Distant metastasis is staged as M1,
and the overall stage grouping consists of stages 1 to 1V.
Stages I and II are considered to be early cancers.
Advanced stages are III and IV cancers.¹¹
Nasopharynx
T1-tumor confined to nasopharynx.
T2-tumor extends to soft tissures of oropharynx and/or nasal fossa.
T2a- Without parapharyngeal extension.
T2b-With parapharngeal extension.
T3-tumor invades bony structures and/or paranasal sinuses.
T4-Tumor with intracranial extension and/or involvement of cranial nerves, infratemporal fossa, hypopharynx, or orbit.8
RADIATION SIDE EFFECTS
Cranial and cervical sympathetic nerve palsey 0.3-6%
Brainstem or cervical spine myelopathy 1%
Hypopituitarism not common but has been reported
Opthalmic side effects after 60Gy - opacities in the lens that develop after several years
Retinopathy with 70 Gy 24-108 months after treatment
Deafness 1%-7%
8% significant hearing impairment
3% bilateral deafness
Osteonecrosis of mandible or maxilla 1%
Dental decay frequently occurs
Xerostomia (moderate or severe) in 75% of patients
IMRT at 4% per Gy exponentially
Trismus 5%-10%
Fibrosis of subcutaneous tissue of the neck with doses of 50Gy 9
Brainstem or cervical spine myelopathy 1%
Hypopituitarism not common but has been reported
Opthalmic side effects after 60Gy - opacities in the lens that develop after several years
Retinopathy with 70 Gy 24-108 months after treatment
Deafness 1%-7%
8% significant hearing impairment
3% bilateral deafness
Osteonecrosis of mandible or maxilla 1%
Dental decay frequently occurs
Xerostomia (moderate or severe) in 75% of patients
IMRT at 4% per Gy exponentially
Trismus 5%-10%
Fibrosis of subcutaneous tissue of the neck with doses of 50Gy 9
PROGNOSIS
Race, age and gender rarely have prognostic significance
T1 lesions local control 90%
T2 lesions local control 85% to 90%
T3 lesions local control 62% to 73%
T4 lesions local control 44% to 71% 10
T1 lesions local control 90%
T2 lesions local control 85% to 90%
T3 lesions local control 62% to 73%
T4 lesions local control 44% to 71% 10
loading Favorite Sites...
TREATMENT
Surgery
Surgery is not an option since the nasopharynx is immiediatly adjacent to the base of the skull. It is impossible to have acceptable margins with surgical resection.
Radical neck dissection has been preformed for neck node metastasis, but this is very rare. (Chao)
Chemotherapy
Neo-adjuvant or adjuvant chemotherapy has been used for primary or recurrent nasopharynx cancer with a complete response rate of 10-20% and partial response rate of 40%.
Cisplatin, Doxorubicin, Epirubicin, Bleomycin and Methotrexate have been shown to be active for this disease. The most effective combinations are cisplatin based.
Radiation Therapy
Opposed laterals are used to treat nasopharynx and adjacent structures.
IMRT provides excellent dose distributions with doses up to 75Gy.
Brachytherapy has been used to deliver a high dose to a limited volume of the nasopharynx and is frequently combined with external irradiation to treat extensive primary or recurrent carcinoma.
Three-dimensional treatment planning and conformal therapy
Proton therapy (Chao)
Treatment Borders
Lateral treatment fields are angled 5 degrees posteriorly to allow coverage of the posterior wall of the nasopharynx while avoiding direct ipsilateral irradiation to the external and middle ear. This also reduces the irradiation to the contralateral lens. The volume to be irradiated includes the nasopharynx, adjacent parapharyngeal tissues (with a 1-2cm margin) and all the cervical lymphatics (jugular, spinal accessory and supraclavicular)
Standard fields should include the posterior ethmoid cells, the posterior 1/3 of the maxillary antrum and the nasal cavity (but not the orbit unless warranted)
Superior border-splits the pituitary fossa and extends anteriorly along the sphenoid plate
Superior border (for base skull involvement)-1cm above pituitary fossa
Anterior border-includes the posterior 2cm of the nasal cavity and maxillary antrum, the clivus is included with a 1cm margin
Anterior border (extension)-the anterior border is moved forward 2cm to cover extension into the ethmoid/maxillary sinuses and occasional into the posterior orbit if warranted.
Posterior border-is behind the cervical processes and should cover the mastoid and occipital lyph nodes
Boost field-after 45Gy the posterior border is moved anteriorly to shield the spine. A higher energy photon should preferably be used. The posterior neck fields is supplemented with 5-15Gy with 9MeV electrons through small lateral fields.
An anterior field can occasionally be added to irradiate anterior tumor extension.
Lower neck and supraclavicular fossa are electively treated with a single anterior field to 50Gy given dose (45Gy at 3cm) with 2Gy daily fractions.
Doses
T1-T2 ----- 65Gy
T3-T4 ----- 70-75Gy
45Gy reduce field to exclude spinal cord then boost to 22-27Gy
T3-T4 ----- 50Gy for young adults age 15-30
Children older than 15 years of age, boost 10-15Gy to regional lymph nodes
Brachytherapy: 5-25Gy (calculated to 0.5-1.0cm) combined with external radiation 11
Surgery is not an option since the nasopharynx is immiediatly adjacent to the base of the skull. It is impossible to have acceptable margins with surgical resection.
Radical neck dissection has been preformed for neck node metastasis, but this is very rare. (Chao)
Chemotherapy
Neo-adjuvant or adjuvant chemotherapy has been used for primary or recurrent nasopharynx cancer with a complete response rate of 10-20% and partial response rate of 40%.
Cisplatin, Doxorubicin, Epirubicin, Bleomycin and Methotrexate have been shown to be active for this disease. The most effective combinations are cisplatin based.
Radiation Therapy
Opposed laterals are used to treat nasopharynx and adjacent structures.
IMRT provides excellent dose distributions with doses up to 75Gy.
Brachytherapy has been used to deliver a high dose to a limited volume of the nasopharynx and is frequently combined with external irradiation to treat extensive primary or recurrent carcinoma.
Three-dimensional treatment planning and conformal therapy
Proton therapy (Chao)
Treatment Borders
Lateral treatment fields are angled 5 degrees posteriorly to allow coverage of the posterior wall of the nasopharynx while avoiding direct ipsilateral irradiation to the external and middle ear. This also reduces the irradiation to the contralateral lens. The volume to be irradiated includes the nasopharynx, adjacent parapharyngeal tissues (with a 1-2cm margin) and all the cervical lymphatics (jugular, spinal accessory and supraclavicular)
Standard fields should include the posterior ethmoid cells, the posterior 1/3 of the maxillary antrum and the nasal cavity (but not the orbit unless warranted)
Superior border-splits the pituitary fossa and extends anteriorly along the sphenoid plate
Superior border (for base skull involvement)-1cm above pituitary fossa
Anterior border-includes the posterior 2cm of the nasal cavity and maxillary antrum, the clivus is included with a 1cm margin
Anterior border (extension)-the anterior border is moved forward 2cm to cover extension into the ethmoid/maxillary sinuses and occasional into the posterior orbit if warranted.
Posterior border-is behind the cervical processes and should cover the mastoid and occipital lyph nodes
Boost field-after 45Gy the posterior border is moved anteriorly to shield the spine. A higher energy photon should preferably be used. The posterior neck fields is supplemented with 5-15Gy with 9MeV electrons through small lateral fields.
An anterior field can occasionally be added to irradiate anterior tumor extension.
Lower neck and supraclavicular fossa are electively treated with a single anterior field to 50Gy given dose (45Gy at 3cm) with 2Gy daily fractions.
Doses
T1-T2 ----- 65Gy
T3-T4 ----- 70-75Gy
45Gy reduce field to exclude spinal cord then boost to 22-27Gy
T3-T4 ----- 50Gy for young adults age 15-30
Children older than 15 years of age, boost 10-15Gy to regional lymph nodes
Brachytherapy: 5-25Gy (calculated to 0.5-1.0cm) combined with external radiation 11
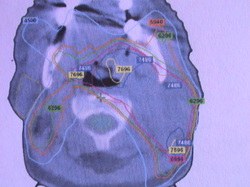
PLANING PICTURES
|
|
TD5/5
SPINAL CORD
According to RTOG 0619 a volume of spinal cord larger than about 3x3x3 mm cubed would be better off having dose less than 48 Gy. Also, in non-IMRT plans any field recieving more than 40-44Gy are to have a spinal block to reach this goal.12
Phillips who invented the NSD curve used his formula to postulate that a limit of 5000cGy was appropriate because anything above this threshold would cause radiation myelitis. Boden recognized the need for volume data when evaluating dose to the spine. A recommendation by Emami is 5500cGy to a volume of 5cm for the TD5/5.13
BRAIN STEM
Bodin and Sheline have made suggestions of what the dose tolerance should be for the brain stem, however Emami believes them to be to conservative and has come up with their own theory of what the dose should be. Emami believes it should be 6000cGy for a volume of 1/3 with an ending result of necrosis.13 According to RTOG the brain stem can recieve, "54Gy or 1% of PTV cannot exceed 60Gy."14
OPTIC CHIASM
Emami decided that the appropriate TD5/5 is 50Gy due to the article written by Hammer who reported that patients who had pituitary tumors developed chiasmal necrosis after receiving 4250cGy in large fractions of 210-280cGy.15 According to RTOG the optic chiasm can recieve, "54Gy or 1% of PTV cannot exceed 60Gy."16
OPTIC NERVE
Many articles such as Parsons, Brown, and Pezner have written articles on optic nerve and blindness. Blindness was found to have occured at or below 50Gy so Emami could not justify to follow some article with the TD5/5 to be 55Gy, instead they decided to follow the TD5/5 of 50Gy.17
According to RTOG the optic nerve can recieve, "54Gy or 1% of PTV cannot exceed 60Gy."18
RETINA
The dose response curve for retina is extremely steep between 50Gy and 60Gy, so according to Emami a realistic TD5/5 is 45 Gy with an ending side effect of visual loss.19
LENS
Emami states that 10Gy should be the TD5/5, but this is concluded after a Seattle group known as Deeg who checked TBI patients post irradiation for the incidences of cataracts.19
MANDIBLE
In some cases the end point is necrosis, however Emami uses Osteoradionecrosis as an endpoint for determining the TD5/5 because of its significants in morbidity. Even though there is no reliable data on volume and dose to the mandible Emami believes that 1/3 should recieve 65Gy or less or anything above this volume should recieve 60Gy and below.19According to RTOG the mandible can recieve, "70Gy or 1cc of PTV cannot exceed 75Gy."20
PAROTID
Emami has made an attempt to determine from literature and clinical experience what the TD5/5 should be for the parotid glands before xerostomia occurs, The TD5/5 they determined is 32Gy with the note that no significant change occurs with less than 50% of the parotid being irradiated.21 "Mean dose is less than or equal to 26Gy in at least one gland or at least 20cc of the combined volume of both parotid glands will receive less than 20Gy or at least 50% of the gland will recieve less than 30Gy in at least one gland." 22
According to RTOG 0619 a volume of spinal cord larger than about 3x3x3 mm cubed would be better off having dose less than 48 Gy. Also, in non-IMRT plans any field recieving more than 40-44Gy are to have a spinal block to reach this goal.12
Phillips who invented the NSD curve used his formula to postulate that a limit of 5000cGy was appropriate because anything above this threshold would cause radiation myelitis. Boden recognized the need for volume data when evaluating dose to the spine. A recommendation by Emami is 5500cGy to a volume of 5cm for the TD5/5.13
BRAIN STEM
Bodin and Sheline have made suggestions of what the dose tolerance should be for the brain stem, however Emami believes them to be to conservative and has come up with their own theory of what the dose should be. Emami believes it should be 6000cGy for a volume of 1/3 with an ending result of necrosis.13 According to RTOG the brain stem can recieve, "54Gy or 1% of PTV cannot exceed 60Gy."14
OPTIC CHIASM
Emami decided that the appropriate TD5/5 is 50Gy due to the article written by Hammer who reported that patients who had pituitary tumors developed chiasmal necrosis after receiving 4250cGy in large fractions of 210-280cGy.15 According to RTOG the optic chiasm can recieve, "54Gy or 1% of PTV cannot exceed 60Gy."16
OPTIC NERVE
Many articles such as Parsons, Brown, and Pezner have written articles on optic nerve and blindness. Blindness was found to have occured at or below 50Gy so Emami could not justify to follow some article with the TD5/5 to be 55Gy, instead they decided to follow the TD5/5 of 50Gy.17
According to RTOG the optic nerve can recieve, "54Gy or 1% of PTV cannot exceed 60Gy."18
RETINA
The dose response curve for retina is extremely steep between 50Gy and 60Gy, so according to Emami a realistic TD5/5 is 45 Gy with an ending side effect of visual loss.19
LENS
Emami states that 10Gy should be the TD5/5, but this is concluded after a Seattle group known as Deeg who checked TBI patients post irradiation for the incidences of cataracts.19
MANDIBLE
In some cases the end point is necrosis, however Emami uses Osteoradionecrosis as an endpoint for determining the TD5/5 because of its significants in morbidity. Even though there is no reliable data on volume and dose to the mandible Emami believes that 1/3 should recieve 65Gy or less or anything above this volume should recieve 60Gy and below.19According to RTOG the mandible can recieve, "70Gy or 1cc of PTV cannot exceed 75Gy."20
PAROTID
Emami has made an attempt to determine from literature and clinical experience what the TD5/5 should be for the parotid glands before xerostomia occurs, The TD5/5 they determined is 32Gy with the note that no significant change occurs with less than 50% of the parotid being irradiated.21 "Mean dose is less than or equal to 26Gy in at least one gland or at least 20cc of the combined volume of both parotid glands will receive less than 20Gy or at least 50% of the gland will recieve less than 30Gy in at least one gland." 22
