BLADDER
WIN REMARKABLE OPPORTUNITIES
BY FOLLOWING SPONSORS LINKS
EPIDEMIOLOGY
Bladder
cancer is the fourth most common cancer in men and the eighth most
common in women. The highest rates of bladder cancer appear in Western
Europe and North America; low rates are found in Eastern Europe and
areas of Asia (China, India, Philippines). Bladder Cancer primarily
occurs in older white men. The incidence in black men is approximately
50% less than white men. Two thirds of bladder cancer cases occur among
people over 65 years old. 6
ETIOLOGY
Major
risk factors for bladder cancer include smoking and occupational
exposures. Smoking increases the risk of bladder cancer two to three
folds. Occupational exposures to aromatic amines in British dyestuff,
rubber, leather, paint and possibly drivers (increased exposure to
exhaust emissions) have been associated with bladder cancer development.
It is suggested that chlorinated organic compounds formed as a
byproduct of drinking water chlorination may be a causative factor.
Exposure to S. haeatobium is associated with an increased risk
of squamous cell carcinoma of the bladder, heavy consumption of
phenacetin- containing analgesics and cyclophosphamide and pelvic
irradiation have also been linked to bladder cancer. 6
loading Favorite Sites...
SIGN & SYMPTOMS
Most patients with bladder cancer,
75%-80%, present with gross painless hematuria. Clotting and urinary
retention may occur. Approximately 25% of patients have symptoms of
vesical irritability, although almost all patients with carcinoma in
situ experience frequency, urgency, dysuria, and hematuria. 3
DIAGNOSTC PROCEDURES
In addition to a complete history
and physical examination, including rectal and pelvic examination, each
patient should have a chest x-ray examination, urinalysis, complete
blood cell count, liver function tests, cystoscopic evaluation, and
bimanual examination performed under anesthesia. Biopsy is done for
diagnosis. An intravenous pyelogram should be evaluated before
retrograde pyelogram, ureteroscopy, brush biopsy, and cytology if
indicated. CT and MRI is uded to evaluate bladder-wall thickening and
detect extravesical extension and lymph node metastases. Bone scans are
obtained for patients with T3 and T4 disease and those with bone pain. 3
HISTOLOGY
Most bladder cancers (98%) are
epithelial in orgin. In the western hemisphere approximately 92% of
epithelial tumors are transitional cell carcinomas, 6% to 7% are
squamous cell carcinomas, and 1%-2% are ademocarcinomas. 3
LYMPH NODE DRAINAGE
The bladder's lymphatic drainage is by the external and internal iliac and presacral lymph nodes.1
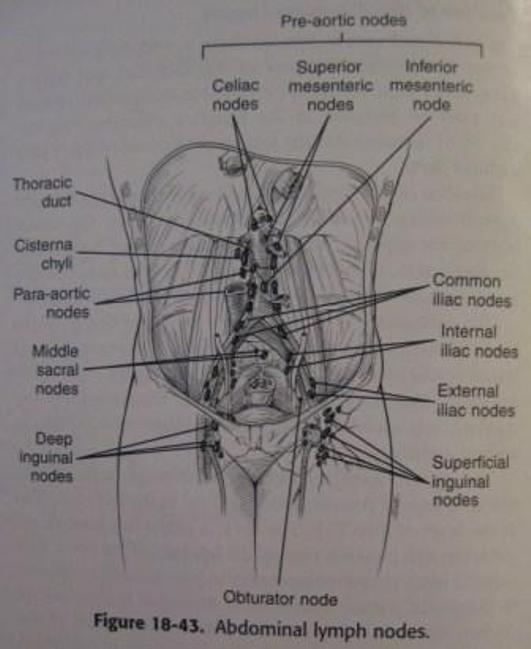
Figure 1. Abdominal lymph nodes.3
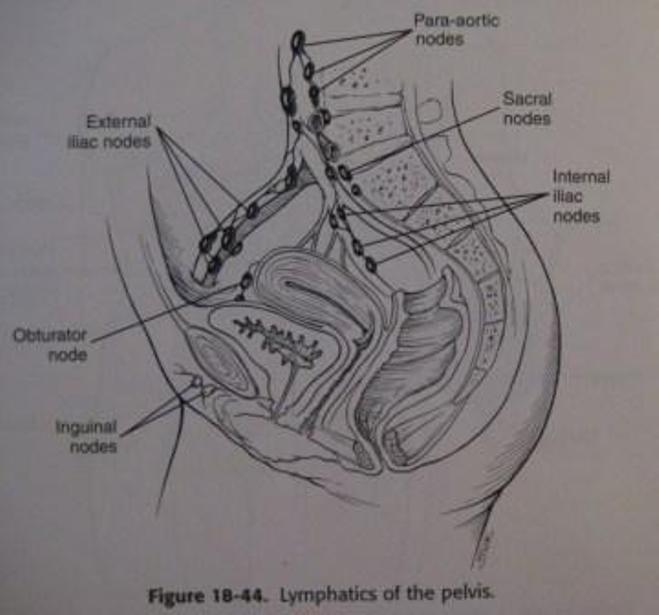
Figure 2. Pelvic lymph nodes.3
METASTATIC SPREAD
Bladder
cancer can spread through direct extension into or even through the
bladder wall. "Intraepithelial involvement of the distal ureters,
prostatic urethra, and periurethral prostatic ducts is frequently found
with multifocal or diffuse carcinoma in situ." Of new bladder cancers,
approximately 75% to 85% are superficial and approximately 15% to 25%
have evidence of muscle invasion at diagnosis. "Perineural invasion and
lymphatic or blood vessel invasion are common after the tumor has
invaded muscle.3 The most common places for distant metastases to occur with bladder cancer are lung, bone, and liver.1
GRADING
The most common grading system uses three grades. These are:
Grade 1--Low grade
Grade 2--Moderate grade
Grade 3--High grade
Low grade means that they look a lot like normal bladder cells a represent cells that are slower growing and less likely to spread. High grade tumors have cells that look very abnormal and represent cells that grow quickly and are more likely to spread. Carcinoma in situ (CIS) of the bladder is always high grade.2
Grade 1--Low grade
Grade 2--Moderate grade
Grade 3--High grade
Low grade means that they look a lot like normal bladder cells a represent cells that are slower growing and less likely to spread. High grade tumors have cells that look very abnormal and represent cells that grow quickly and are more likely to spread. Carcinoma in situ (CIS) of the bladder is always high grade.2
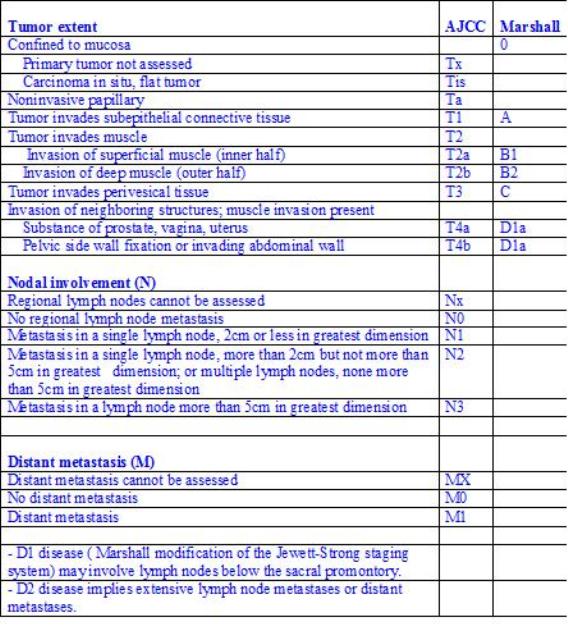
STAGING
There
are two clinical staging system widely used in the US for bladder
cancer. They are the Marshall modification of the Jewett-Strong system
and the tumor-node-metastasis (TNM) staging system of the American Joint
Committee on Cancer.1 Both systems are based on the clinical findings from examination and TUR specimens. See comparison figure 3 below. 1
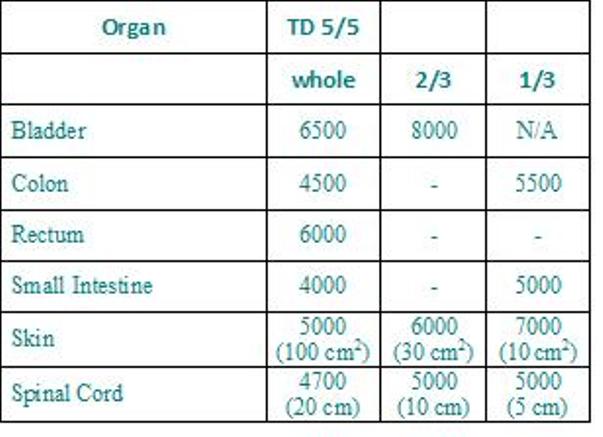
RADIATION SIDE EFFECTS
The
most common acute side effects of radiation include nausea, vomiting,
abdominal cramps, cystitis (10% patients), and diarrhea . Bladder
contracture occurs in 1% of patients. Morbidity is associated with
complications of the bladder (8-10%), rectum(3-4%), and small bowel
(1-2%) from radical irradiation. Late radiation complications attribute
to the 1% mortality rate.1
PROGNOSIS
Prognostic factors for bladder cancer include: depth of tumor invasion and grade. Lymphatic
and blood vessel invasion is a significant indicator even without the
presence of positive lymph nodes or confined to lamina propria.
Poor prognostic indicators include: carcinoma in situ, solid tumor morphology, bulky tumor size, large number of tumors, positive lymph nodes, and obstructive uropathy. 1
Poor prognostic indicators include: carcinoma in situ, solid tumor morphology, bulky tumor size, large number of tumors, positive lymph nodes, and obstructive uropathy. 1
loading Favorite Sites...
TREATMENT
Gerneral Management:
Radiation Therapy Technique:* A four-field box technique with the patient supine is frequently used. It is sometimes helpful to use wedges in the lateral fields to improve dose homogeneity throughout the volume.
- Ta and T1 tumors are usually treated by transurethralresection, TUR, and fulguration, breakdown of tissue via intense electronic sparks, with or without chemotherapy or bacille Calmette-Guérin.
- Most commonly used agents are thiotepa, mitomycin C, doxorubicin, and bacille Calmette-Guérin.
- Patients with diffused grade 3, T1 disease or involvement of the prostatic urethra or ducts are sometimes treated with cystectomy.
- For carcinoma in situ, prompt radical cystectomy is usually curative, but most patients and urologists perfer more conservative initial management, which is TUR and fulguration of visible lesions.
- Patients with muscle-invasive or superficial tumors not suitable for TUR may be treated by segmental resection, partial cystectomy.
- For superficial disease (Tis, Ta, T1) when conservative treatment is unsuccessful, radical cystectomy (without preoperative radiation) is recommended. Cystectomy is also recommended for patients with clinical stage T2-3 disease and for recurrent tumors in patients with less than adequate bladder capacity.
- If no preoperative radiation or only a low dosage of radiation like 20 Gy is given, lymphadenectomy is generally performed for patients with muscle-invasive tumors.
- A lymphadenectomy is usually not performed when a patient has received a preoperative radiation dose of 45- 50 Gy.
- Preoperative radiation is recommended for tumors 4 cm or larger, deeply infiltrating tumors (T3 and resectable T4), or high-grade lesions because of the risk of serious understaging in these cases is high.
- For patients who are medically inoperable, refuse cystectomy, or have disease that is too advanced for surgery, radiation is given.
- A combination of pre and post-op, the sandwich technique, has been used at some institutions.
- A bladder preservation regimen for T2-4a tumors used in selected patients has included maximal TUR bladder tumor resection and two cycles of neoadjuvant chemotherapy (methotrexate, cisplatin, and vinblastine), followed by a pelvic radiation dosage of 39.6- 45 Gy with concomitant cisplatin. Cystoscopy and biopsies are performed. Patients with negative postinduction therapy biopsies receive consolidative chemoirradiation to a total of 64.8 Gy with reduced portals.
- Interstitial treatment may be used alone, in combination with low- or moderate-dose external-beam radiation, or to treat the suture line in patients undergoing partial cystectomy. Suitable patients are those with solitary T1, T2, or T3 lesions measuring less than 5 cm whose general medical condition permits suprapubic cystotomy.
Radiation Therapy Technique:* A four-field box technique with the patient supine is frequently used. It is sometimes helpful to use wedges in the lateral fields to improve dose homogeneity throughout the volume.
- Other techniques, such as AP/PA, rotational, and three-field, have also been used.
- The superior border is usually at the middle of the sacroiliac joint or, depending on the extent of the disease, it may be as high as the L-5- SI junction.
- The inferior border is usually at or just below the bottom of the obturator foramen unless there is diffuse involvement of the bladder neck or prostatic urethra with carcinoma in situ, in which case the borders are extended to the bottom of the ischial tuberosities.
- The regional lymph nodes are treated by including the bony pelvic side walls with approximately a 1.5-cm margin in the AP/PA fields.
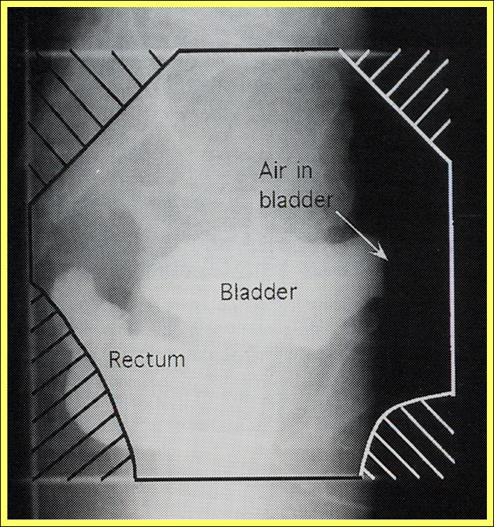
- On the lateral fields, the posterior border is set at least 3 cm behind the posterior bladder wall. If tumor extends posteriorly beyond the vesical wall, the border in set 3 cm behind the tumor mass as determined by palpation or computed tomography scan. It is usually possible to exclude the posterior half of the rectum.
- The anterior border of the lateral fields is placed just in front of the bladder. The blocking prevents falloff over the anterior skin surface.
- Because of varying degrees of bladder distention, the cancer is a "moving target." Depending on what one wishes to accomplish, the bladder may be treated empty or full. In most patients initial treatment volume, which generally covers the entire bladder, is kept as small as possible by having the patient void before treatment. For patients with tumor confined to the bladder base or neck region, the reduced fields, which often include only the involved portion of the bladder, are sometimes treated with the bladder full to displace the small bowel out of the pelvis region.
- A reduced field is done after 45- 50.4 Gy (1.8 Gy/fraction).
- Total tumor dose with radiation alone is 64.8- 68.4 Gy.
- For pre-op radiation, doses are 30 Gy in 10 fractions over 2 weeks or 44 Gy in 22 fractions over 4.5 weeks, followed by a cystectomy in 2- 4 weeks.
- Treatment is preferable with high-energy photons, like 10- 20 MeV. 1
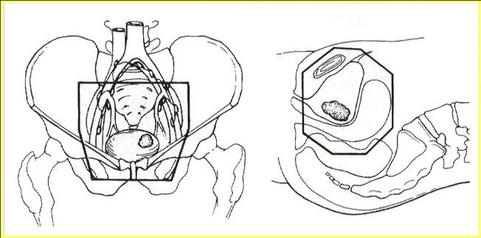
AP/PA and Lateral fields for carcinoma of the bladder 5
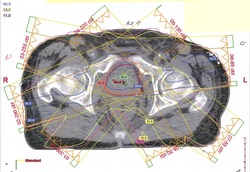
PLANING PICTURES
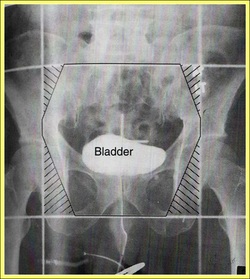
AP treatment port film 5
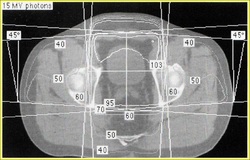
Example of a 4-field box plan for carcinoma of the bladder 5
|
Example of an IMRT plan for carcinoma of the bladder
|
TD5/5